|
Retroperitoneal Fibrosis
· General considerations
o Relatively uncommon
o More common in males than in females
o Predominantly patients aged 40-60 years
o In almost 70% of patients, no cause is found
· Primary or Idiopathic Retroperitoneal Fibrosis (RPF)
o May be an autoimmune response to ceroid, an insoluble lipid that can leak through a thinned arterial wall from atherosclerotic plaques
§ Leads to a vasculitis
o Also found in association with other fibrosing diseases suggesting auto-immune mechanism
§ Primary biliary cirrhosis
§ Fibrosing mediastinitis
§ Glomerulonephritis
§ Panhypopituitarism
§ Rheumatoid arthritis
§ Ankylosing spondylitis
§ Polyarteritis nodosa
§ Systemic lupus Erythematosis (SLE)
§ Hashimoto thyroiditis
· Secondary Retroperitoneal Fibrosis
o Has been found associated with certain drugs, such as
§ Methylsergicide
§ Beta-adrenergic blockers
§ Lysergic acid diethylamide (LSD)
§ Methyldopa
§ Amphetamines
§ Phenacetin
§ Hydralazine
§ Cocaine
o Desmoplastic response to malignancy
§ Lymphoma
§ Carcinoid
§ Retroperitoneal metastases (breast, lung, thyroid, GI tract, GU organs)
o Retroperitoneal fluid collection as in trauma, surgery or infection
o Aneurysm of the aorta or iliac arteries (desmoplastic response)
o Radiation therapy
· Pathology
o Mass of whitish, dense, fibrous tissue covering the aorta, vena cava, ureters, and psoas muscles
o Center of disease is usually located at the level of the 4th or 5th lumbar vertebra just at the aortic bifurcation
· Clinical findings
o Most common presentation is flank, back, scrotal or lower abdominal pain
o Fever
o Weight loss
o Nausea and vomiting
o Symptoms relating to renal impairment and hypertension are common clinical features
· Imaging Findings
o On excretory or CT urography
§ Medial deviation of the ureter beginning at the level of the L3 or L4 (DDx: aortic aneurysm, bladder diverticulum, abdominoperineal resection)
· Not a constant feature
· Most retroperitoneal masses displace ureters laterally
§ Proximal ureterectasis and pyelocaliectasis
§ Tapering of ureters distal to mass
o On CT scans
§ Rind of soft tissue around aorta and inferior vena cava between level of kidney and sacrum
§ Spreads to involve the ureters, causing varying degrees of obstruction.
§ Fat plane between the mass and the psoas muscle may be obliterated
§ Unlike adenopathy, RPF tends not to displace aorta anteriorly
§ Mass may show varying degrees of enhancement depending on the stage of the disease
o CT features-benign vs. malignant masses
§ Mass in RPF is less bulky than most neoplastic lesions
§ Malignancy produces enlarged mesenteric nodes and displacement of the aorta from the spine
§ Most retroperitoneal neoplasms displace the ureters laterally
o US
§ Hypoechoic homogeneous mass
o MRI
§ Low to medium homogeneous signal intensity on T1
§ Heterogeneous high signal intensity on T2 (inflammatory stage)
§ Low signal intensity on T2 (dense fibrotic stage)
· Treatment
o Use of steroids in RPF is controversial
o Surgical ureterolysis
o Immunosuppressive drugs
· Prognosis
o Satisfactory if renal impairment is not too severe

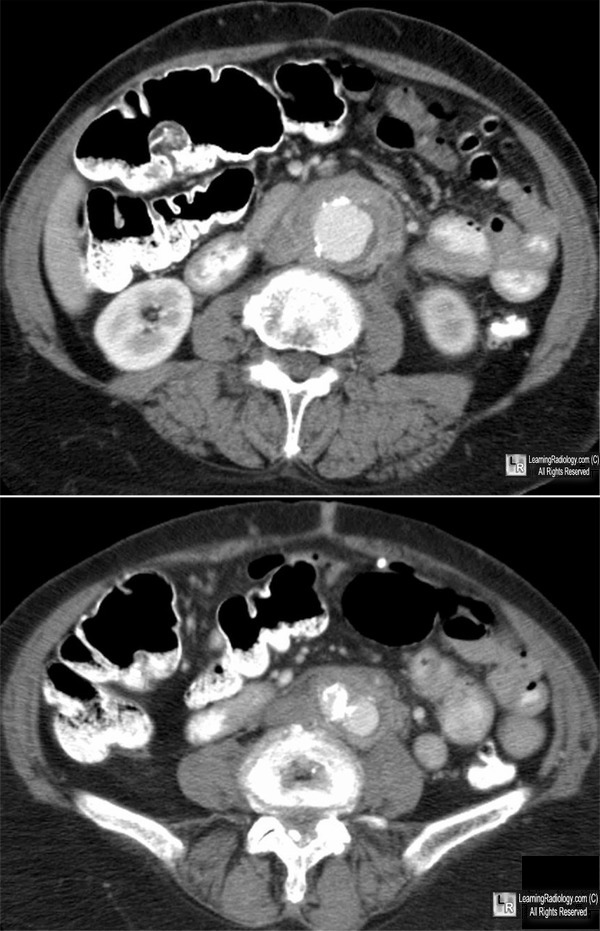
Retroperitoneal Fibrosis. There is a thick rind of soft tissue surrounding the aorta from the level of the kidneys
(top photo-yellow arrow) to and including the bifurcation (bottom photo-red arrow).
The soft tissue enhances slightly. Notice the aorta is not displaced forward as it would more likely be in lymphoma.
The left ureter (green arrow) is dilated.
For these same photos without the arrows, click here
For more information, click on the link if you see this icon 
Ali
Nawaz
Khan,
Muthusamy
Chandramohan
and
Sumaira
Macdonald eMedicine
Dahnert
4th Edition
| 
{kind=link}